The middle phalanx, often overlooked amidst the complex anatomy of the human hand, plays a critical role in both fine motor skills and overall hand function. It forms the middle segment of the three phalanges that make up each finger, situated between the proximal and distal phalanges. Despite its size, its structural integrity and functionality influence a wide array of daily activities, from gripping objects to intricate movements requiring precision. A thorough understanding of the middle phalanx’s anatomy, its biomechanical functions, and the common injuries associated with it is essential for clinicians, anatomists, and rehabilitation specialists dedicated to restoring optimal hand performance after trauma or degenerative processes.
Key Points
- Detailed structural analysis of the middle phalanx highlights its unique features and biomechanical contributions.
- Functional roles extend beyond simple stability, influencing dexterity and force transmission.
- Common injuries include fractures, dislocations, and overuse syndromes, each with specific diagnostic and treatment considerations.
- Advances in imaging modalities improve injury detection and guide management strategies.
- Expert insights emphasize multidisciplinary approaches for comprehensive rehabilitation and recovery.
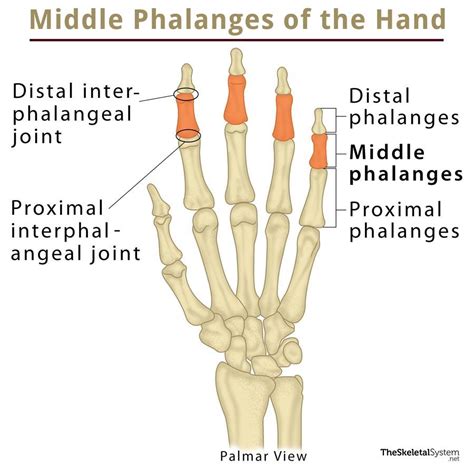
Anatomy of the Middle Phalanx: Structural Composition and Morphology

The middle phalanx is a short, cylindrical bone typically measuring approximately 15 to 20 millimeters in length in adults, though this varies based on finger length and individual anatomical differences. It is characterized by a body that is broader proximally than distally, with two articular surfaces at either end—proximal and distal facets—that articulate with the adjacent phalanges.
Structurally, the bone comprises a dense cortical layer enveloping a trabecular (spongy) interior, which provides resilience to compressive forces encountered during daily activities. The diaphysis, or shaft, exhibits slight curvature, especially in the lesser digits, to facilitate hand ergonomics. Notably, the proximal articular surface features a convex shape that articulates with the proximal phalanx, while the distal end presents a concave surface connected to the distal phalanx.
Variations in morphology are not uncommon, particularly in individuals with certain congenital conditions or developmental adaptations. Also, the volar (palmar) surface tends to be flattened to accommodate flexor tendons, while the dorsal aspect is more convex, aiding in the distribution of mechanical loads.
Biomechanical Functions and Attachments
The middle phalanx serves as a pivotal element in finger biomechanics, acting as a lever during flexion and extension. Its articular surfaces not only establish stability but also facilitate smooth motion across flexion-extension cycles. Major muscular attachments, such as the Flexor digitorum superficialis tendons, originate or insert near this bone, transmitting muscular force necessary for grasping and manipulating objects.
Ligamentous support, especially from the collateral ligaments, stabilizes the joint, preventing excessive lateral movement that could result in dislocation. The integrity of the volar plate, a thick fibrocartilaginous structure on the palmar side, further stabilizes the proximal interphalangeal joint, emphasizing the importance of the middle phalanx's structural robustness.
| Relevant Category | Substantive Data |
|---|---|
| Length in adults | 15-20 mm, varies with digit and individual traits |
| Articular surface shape | Convex proximally, concave distally |
| Bone density | High cortical bone with trabecular interior, approximately 1.2 g/cm³ in healthy adults |

Functional Roles of the Middle Phalanx in Hand Mechanics

The middle phalanx’s primary function centers around joint stability and force transmission. During grasping, finger flexion involves coordinated action starting from the flexor tendons, passing through their attachments at the middle phalanx. This bone acts as a rigid lever, translating muscular effort into functional movement. Moreover, the joint surfaces provide critical range of motion, allowing degrees of flexion that enable pinching, gripping, and delicate manipulation.
From an evolutionary perspective, the middle phalanx’s design reflects a balance between mobility and stability. Notably, the proximal interphalangeal joint (PIP)—the joint between the proximal and middle phalanges—serves as a pivotal hinge, allowing approximately 100 degrees of flexion in the index finger, with slight variations among digits.
Neurovascular Considerations and Sensory Innervation
The middle phalanx is richly supplied by digital arteries and innervated by digital nerves, which provide sensory feedback essential for fine motor control. The dorsal and volar aspects receive different nerve branches, affecting sensation during injury or surgical intervention. An understanding of this neurovascular network guides clinical decisions to preserve function during traumatic or surgical management.
Common Injuries and Pathologies of the Middle Phalanx
Despite its sturdy construction, the middle phalanx is susceptible to various injuries, often resulting from trauma, overuse, or degenerative processes. These injuries can significantly impair hand function if not diagnosed early and managed appropriately.
Fractures of the Middle Phalanx
Fractures are among the most prevalent injuries, with axial and diaphyseal fractures accounting for approximately 60% of middle phalanx injuries. They typically occur from direct trauma, such as a crush injury or a fall onto the finger tip.
The classification of these fractures hinges on factors such as displacement, angulation, and intra-articular involvement. Notably, non-displaced fractures generally heal well with conservative treatment, whereas displaced or intra-articular fractures may require surgical fixation to prevent malunion or joint stiffness.
Dislocations and Ligamentous Injuries
Dislocation at the proximal interphalangeal joint often involves disruption of the collateral ligament complexes. Posterior dislocation is the most common, caused by hyperextension trauma, and can lead to instability if not properly reduced. Ligament injuries may also manifest as sprains, especially in athletes engaged in gripping activities.
Overuse and Degenerative Conditions
Chronic overuse, especially in manual laborers or individuals engaging in repetitive finger movements, can lead to degenerative joint disease affecting the middle phalanx. Symptoms include pain, swelling, and decreased range of motion, complicating hand function over time.
Diagnostic Strategies and Imaging Modalities
Accurate diagnosis of middle phalanx injuries relies heavily on a combination of clinical evaluation and imaging. Standard radiographs remain the first-line modality, providing detailed visualization of fractures and dislocations. For complex or occult injuries, MRI offers superior soft tissue contrast, revealing ligamentous or cartilaginous involvement that plain films may miss.
Computed tomography (CT) scans, especially with 3D reconstructions, facilitate precise fracture mapping—crucial in preoperative planning. Ultrasound serves as a real-time, dynamic tool, particularly useful for assessing ligament integrity or guiding minimally invasive procedures.
Management Approaches and Rehabilitation

Conservative treatment, including immobilization with splints or buddy taping, suffices for most non-displaced fractures and minor ligamentous injuries. However, displaced fractures, open injuries, or intra-articular involvement typically warrant surgical intervention, such as pinning, plating, or fixation with mini-screws.
Post-treatment rehabilitation emphasizes early motion exercises to prevent stiffness and promote joint mobility. Hand therapy involving range of motion and strengthening exercises plays a crucial role in restoring functional capacity, especially after complex surgeries.
Evolutionary and Functional Significance
The design of the middle phalanx reflects a remarkable evolutionary refinement aligning with humans’ unique manual dexterity. Its structural simplicity disguises a complex interplay of biomechanics that enables nuanced movements critical for tool use, communication, and social interaction.
Historically, deformities or injuries of the middle phalanx have been documented in artifacts from ancient civilizations, indicating the importance placed on hand function even millennia ago. Contemporary research continues to explore optimizing restorative procedures, driven by the understanding that the middle phalanx's health is central to hand functionality.
Forward-Looking Perspectives in Middle Phalanx Research
Ongoing studies aim to develop biomaterials mimicking bone properties for fracture repair, as well as regenerative therapies to restore damaged ligamentous structures. The integration of robotic-assisted surgeries and digital modeling promises to enhance surgical precision and predict post-operative outcomes.
Meanwhile, understanding the influence of systemic factors, such as osteoporosis and diabetes, on healing trajectories remains a priority for clinicians aiming to tailor individualized treatments.
What are the typical signs of a fracture in the middle phalanx?
+Signs include localized swelling, pain on movement or palpation, deformity, and sometimes bruising. Patients may also experience difficulty flexing or extending the finger, along with tenderness over the bone. Radiographic imaging often confirms the diagnosis.
How can I distinguish between a ligament sprain and a fracture in the middle phalanx?
+Clinically, fractures often present with more localized swelling, crepitus, and a visible deformity, especially if displaced. Imaging studies are essential for differentiation—X-rays can reveal fractures, whereas MRI is more sensitive for ligament injuries without bone damage.
What are the current best practices for rehabilitating a fractured middle phalanx?
+Early stabilization followed by controlled mobilization, guided by hand therapy specialists, promotes optimal healing. For surgical cases, staged rehabilitation involving splinting initially, then gradual range-of-motion exercises, is common. Emerging approaches also include the use of functional orthoses and digital monitoring to optimize recovery timelines.
Are there any preventive measures to avoid middle phalanx injuries?
+Protective gear during high-impact activities, ergonomic modifications, and strength training of intrinsic hand muscles can reduce injury risk. Educating individuals on proper hand ergonomics and avoiding overexertion in repetitive tasks also plays a vital role in prevention.
What advances are emerging in surgical repair of complex middle phalanx fractures?
+Innovations include minimally invasive fixation techniques, bioresorbable implants, and stem cell-based regenerative therapies aimed at enhancing healing. Additionally, 3D printing of patient-specific implants is gaining traction for complex intra-articular fractures.


