The Lachman test has long stood as a cornerstone assessment within orthopedic sports medicine, particularly in evaluating knee stability and diagnosing anterior cruciate ligament (ACL) injuries. With the increasing prevalence of ACL tears among athletes and generalized populations alike—estimated at approximately 81,000 annually in the United States alone—the importance of precise diagnostic tools like the Lachman test cannot be overstated. Understanding the biomechanics, proper execution, and interpretive nuances of this test offers invaluable insights into knee joint integrity. Moreover, its application extends beyond diagnosis, serving as a guide for injury prevention strategies, rehabilitation protocols, and ultimately, return-to-play decisions. This comprehensive examination synthesizes current evidence, clinical expertise, and emerging research to elucidate the Lachman test's role in promoting knee health, safeguarding athletes, and optimizing clinical outcomes.
Key Points
- The Lachman test remains a highly sensitive diagnostic tool for ACL integrity, with reported sensitivities exceeding 90% in expert hands.
- Proper technique emphasizes specific patient positioning, force application, and interpretation of translation, influencing diagnostic accuracy.
- Biomechanical insights reveal that the anterior tibial translation measured during the test correlates with ACL integrity, providing quantifiable data for clinical decision-making.
- Risk mitigation protocols incorporating neuromuscular training and biomechanical assessment can reduce incidence rates of ACL injuries, especially among high-risk populations.
- Emerging innovations such as robotic-assisted evaluation and advanced imaging complement traditional Lachman testing, enhancing diagnostic precision.
Biomechanics of the Knee and the Significance of the Lachman Test

The human knee embodies a complex hinge joint stabilized by a web of ligaments, tendons, and musculature. Among these, the anterior cruciate ligament (ACL) plays a pivotal role in preventing anterior tibial translation relative to the femur. Anatomically, the ACL comprises two bundles—anteromedial and posterolateral—that work synergistically to maintain joint stability across various ranges of motion. Disruption of this ligament leads to increased anterior laxity, predisposing individuals to functional instability, meniscal injuries, and early osteoarthritis.
The Lachman test serves as a biomechanically grounded clinical maneuver designed to physiologically quantify this anterior tibial translation. When executed accurately, it isolates the ACL's contribution to joint stability by resisting soft tissue and capsular structures, providing a direct assessment of ligament integrity. The test's sensitivity hinges on its capacity to reproduce clinical laxity that reflects underlying ligamentous injury, thus acting as a surrogate for more invasive or imaging-based evaluations.
Mechanics and Execution of the Lachman Test
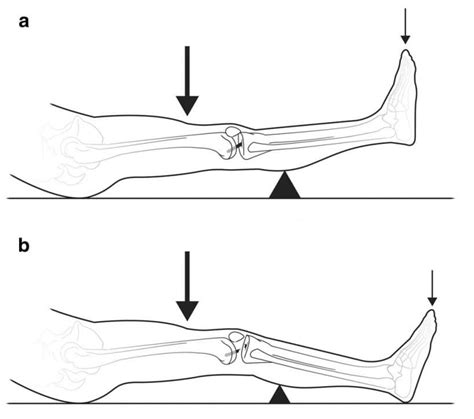
The Lachman test involves positioning the patient supine on an examination table, with the knee flexed approximately 20-30 degrees—an angle optimized for maximal ACL tension and ease of palpation. The clinician stabilizes the distal femur with one hand while gripping the proximal tibia with the other, exerting a gentle anterior force to assess tibial translation relative to the femur.
Critical to the test’s validity is the application of consistent force, the avoidance of unnecessary movement, and the interpretation of what constitutes normal versus abnormal translation. A translation exceeding 3 mm on lateral translation devices or the clinician’s judgment typically indicates an ACL tear. In addition, a soft or absent end-point during anterior translation further signifies compromised ligamentous continuity. High inter-rater reliability, especially among experienced clinicians, underscores the test’s robustness when performed methodically.
| Relevant Category | Substantive Data |
|---|---|
| Sensitivity and Specificity | Over 90% sensitivity and 94% specificity reported in expert hands for ACL tears |
| Average anterior tibial translation in healthy knees | Approximately 2-3 mm; increased beyond 3-4 mm suggests injury |
| Reproducibility concerns | Operator experience influences accuracy; standardized protocols improve reliability |

Understanding Knee Stability and Injury Prevention

In the broader context, knee stability hinges on the integrity of ligaments like the ACL, PCL, MCL, and LCL, as well as neuromuscular control mechanisms. For athletes and active individuals, the risk factors for ACL injury encompass biomechanical, neuromuscular, and environmental components. Recent epidemiological data demonstrate that female athletes experience ACL injuries at approximately 2-8 times higher rates than males in comparable sports, attributable to anatomical differences, hormonal influences, and neuromuscular factors.
Injury prevention programs have evolved from purely strength-based training to comprehensive neuromuscular and proprioceptive interventions. Such programs aim to reinforce dynamic knee stability, reduce excessive anterior tibial translation, and refine landing mechanics. The role of the Lachman test in this preventive paradigm is twofold: it serves as a screening tool for laxity and guides clinicians in identifying individuals at heightened risk who may benefit from targeted interventions.
Implementing Evidence-Based Prevention Protocols
Numerous studies substantiate the efficacy of prevention programs in reducing ACL injury incidence. For example, the PEP (prevent injury and enhance performance) program, integrating plyometrics, balance training, and strength exercises, has demonstrated a reduction of ACL injuries by up to 52% in high school female athletes. While these interventions focus on neuromuscular control and biomechanical correction, the Lachman test functions as a secondary assessment to monitor changes in knee stability over time.
Beyond screening, early detection of increased anterior laxity via the Lachman test during preseason evaluations may prompt the implementation of personalized preventive strategies, including neuromuscular training adjustments, footwear modifications, and activity modifications if necessary.
Limitations, Challenges, and Future Directions
Despite its strengths, the Lachman test is not without limitations. Factors such as acute swelling, pain, or patient guarding can obscure assessment accuracy. Inter-rater reliability variances underline the necessity for standardized training and possibly adjunctive objective measures.
Emerging technologies aim to address these shortcomings. Robotic-assisted devices and portable arthrometers provide quantifiable translation measurements, reducing subjective bias inherent in manual testing. Furthermore, advanced imaging modalities—like MRI—complement clinical assessment by visualizing ligamentous structure and surrounding tissues, facilitating comprehensive diagnosis.
Concluding Perspectives: From Diagnosis to Injury Prevention
The Lachman test remains an enduring instrument in the clinician’s armamentarium for evaluating knee stability, especially concerning ACL integrity. Its biomechanical foundation, combined with evolving adjunctive technologies, reinforces its central role in both diagnostics and injury prevention. By accurately assessing anterior tibial translation, medical professionals can not only diagnose injuries with high confidence but also proactively identify individuals at risk. As research continues to refine our understanding of knee biomechanics and the interplay of neuromuscular factors, the Lachman test’s utility will likely expand, supported by technological advancements that mitigate its current limitations.
How does the Lachman test compare to other knee stability assessments?
+The Lachman test is generally regarded as more sensitive and specific than the anterior drawer test, especially in acute settings. Its position at approximately 20-30 degrees of flexion captures ACL integrity effectively, whereas other tests like the pivot shift or Lachman have different evaluative focuses for various ligamentous structures.
What are common pitfalls when performing the Lachman test?
+Common issues include improper knee flexion angle, excessive force leading to patient discomfort, inconsistency in palpation, or misinterpretation of translational movement. Ensuring proper technique, patient relaxation, and clinician training minimizes these errors.
Can the Lachman test be used in chronic knee instability?
+Yes, the Lachman test remains valuable in chronic cases. However, tissue remodeling, scar formation, and altered biomechanics may affect its sensitivity. Combining it with imaging and functional assessments offers a more comprehensive understanding of persistent instability.
Are there technological advancements that improve Lachman test reliability?
+Emerging device-assisted arthrometers provide objective measures of anterior tibial translation, thus reducing the subjective variability of manual testing. These tools enhance reproducibility and can be particularly useful in research settings or for longitudinal patient monitoring.
What role does neuromuscular training play alongside Lachman testing in injury prevention?
+Neuromuscular training improves joint proprioception, muscle coordination, and landing mechanics, which collectively reduce ACL injury risk. Regular assessment using the Lachman test can help track improvements or identify residual laxity warranting targeted interventions.